Gastrointestinal Foreign Body by Jeremy Fleming, DVM, DACVS-SA
Dinky was a 4 year old, male neutered Grate Pyrenees Mix who was adopted by his owners approximately 5-6 months prior to presentation. The owners described him to be more independent than their other large breed dogs and has always had abnormal defecations. He was reported to have straining during defecation and only produced small, egg shaped, hard/dry feces. He would occasionally vocalize and cry out when straining. He seemed uncomfortable/panting after these episodes. He was otherwise eating, drinking, and urinating well with no vomiting or diarrhea noted.
He was initially seen by a primary care veterinarian where a fecal test was negative and was started on probiotics and metronidazole. Initial medical therapy was unsuccessful. Mineral oil was started orally which also did not help improve clinical signs.
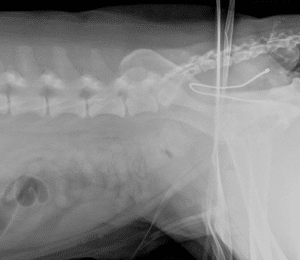
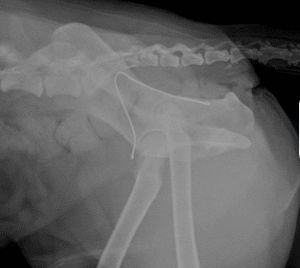
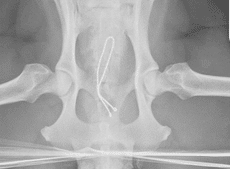
He was then taken to the referring veterinarian where rectal examination revealed a metallic, wire-like foreign body in the distal rectum extending proximally beyond digital palpation. Sedated radiographs were taken and showed a wire foreign body in the pelvic canal with looped ends. Gentle rectal traction was performed but the wire felt imbedded in mucosal tissue and was abandoned.
Dinky was then presented through Austin Veterinary Emergency and Specialty Center Emergency Department for further evaluation. Initial vital signs and general physical examination were within normal limits with exception of the rectal examination. Rectal exam revealed a wire ending approximately 2cm to the anus and extending cranially until it ended in rectal mucosa. A second part of the wire could be felt approximately 3cm cranial to the rectum which also had a rounded end. Dinky was then transferred to our Critical Care specialist Dr. Jamie Becker.
Dinky was placed under general anesthesia under guidance of AVES Anesthesiologist, Dr. Whittaker, for colonoscopy with AVES Internal Medicine department and AVES Internal Medicine Specialist Dr. Slead. Colonoscopy showed a single metal wire with penetration through the dorsal left rectal wall at the 11 o’clock position. The U-shape bend was full imbedded in the rectal wall with the wire being seen exiting the rectal wall then re-emerging into the lumen. Both ends of the wire were pointed caudally. Gentile manipulation with endoscopy was attempted but the wire was fully embedded and could not be removed without tearing the rectal wall. Tearing at this location could result in severe complications such as septic peritonitis, recurrent perianal/pelvic abscesses, or rectocutaneous fistula formation.

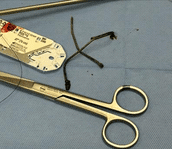
After multi-specialty discussion and a thorough discussion with the owners, Dinky was then taken to Surgery with Dr. Jeremy Fleming, one of our board-certified surgeons. Proctoscopy examination was performed with a SILS port (blue malleable foam Single Incision Laparoscopic Surgery port with three instrument portals) was lubricated and inserted into the rectum. Visualization of the entire luminal portion of the wire was performed using CO2 insufflation through the SILS port. The location of the wire cut was evaluated to be at the mucosal edge of the more caudal luminal penetration. The SILS port was removed. The wire was cut in the appropriate location using digital palpation and insertion of a medium sized wire cutter. The free piece was extracted digitally and the SILS proctoscopy port was placed back in place. Laparoscopic utensils were used to gently guide the U-turn of the wire cranially, similar to removal of a fishhook. Once removed from the colon wall, the second piece of wire was extracted.

After wire extraction, absorbable barbed suture was introduced into the rectal lumen and each puncture hole was sutured closed to help prevent leakage of colonic material and inciting bacterial infection. No incisions were made during this procedure.
Dinky made a full recovery from anesthesia and was discharged from the hospital on the day of surgery. Postoperative medications included Gabapentin, amoxicillin-clavulanic acid, and enrofloxacin. Mineral Oil administration was discontinued.
Dinky made a rapid a full recovery at home. Since discharge, he has had normal defecations without straining, vocalization, or pain. His mentation has improved and he has become less independent and more willing to play with his housemates. The owners report a complete change in his demeanor and significant improvement to his quality of life.
Latest posts by Austin Veterinary Team
(see all)